
Immune System Dysregulation
Your immune system is critical to your well being. Yet these days so many people suffer from allergies, auto immune diseases or cancer.
There are diverse causes and treatments for immune dysregulation, though through a holistic approach you give your body the best chance of putting out the fire of inflammation, resetting the system, and restoring vitality. We create a personalised plan for you, and explain the why behind the why, rather than just trying to treat your symptoms.
We treat all allergies, Mast Cell Activation Syndrome[1] (MCAS), and autoimmune diseases. Book an appointment with Evergreen Doctors today to get you back on the road to wellness.

Chronic Inflammatory Response Syndrome (CIRS)
CIRS is a diagnosis of exclusion, and is characterized by a cluster of symptoms that may include visual disturbances, fatigue, cognitive decline, body aches, mood changes, unusual pains or skin sensations and sinus or breathing difficulties.
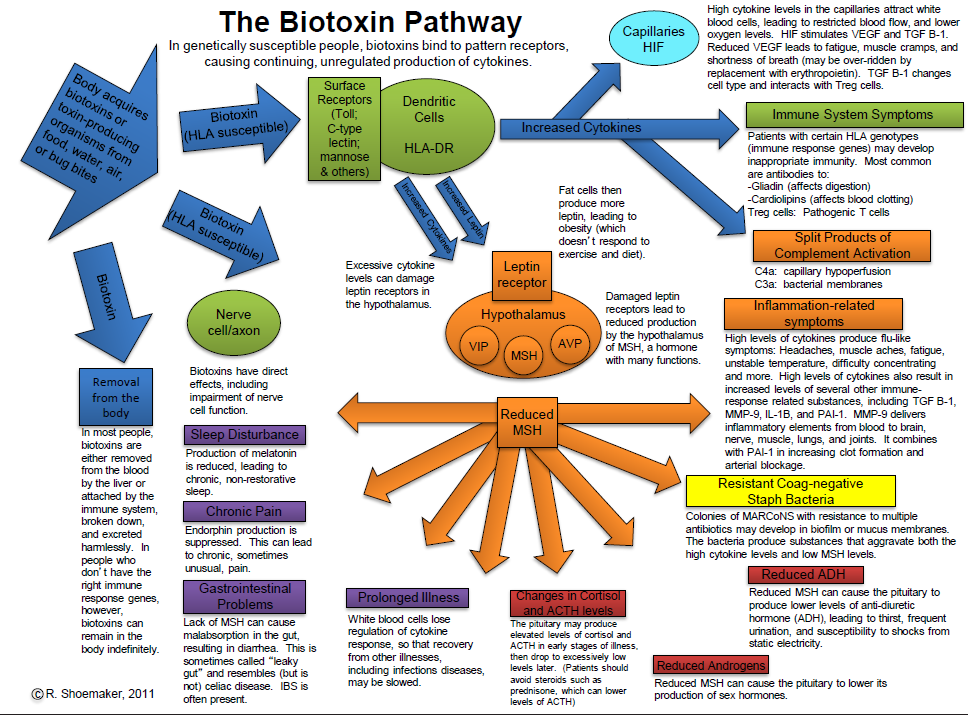
CIRS patients can become more and more ill as time passes if they are being constantly exposed to the triggering agent, or their condition isn’t treated. And thus they develop chronic multiple fluctuating symptoms. It is no use treating individual symptoms and trying to suppress them. The true underlying pathways need to be assessed and treated. This includes removal of the biotoxin or exposure[2], increasing detoxification pathway function and supporting and enhancing mitochondrial function within the cells.
It is vitally important to seek the underlying causal mechanisms and to treat those. What is known is that it is more common in genetically predisposed persons (however, this is 25% of the population!) and those can be tested for in blood panels. The genes that make you susceptible to CIRS are involved in multiple pathways, including important detoxification pathways.
Unfortunately patients with CIRS often get bounced around the health system and spend years without a clear understanding of the cause of their symptoms as they can appear to be quite separate to doctors not familiar with CIRS. It’s very important that no underlying diseases are missed and therefore patients need to have a thorough work up, by a suitability trained doctor. If you do have CIRS and the real causes are found, with the right treatments most patients make a full recovery.
Recent research by Dr Andrew Heyman’s group has found epigenetic changes at the mitochondrial level play a key role in creating a chronic inflammatory state. This results in lipids changing into toxic forms and cell membranes becoming more “sticky” and “leaky”[3]. From this perspective it is not an ongoing exposure or infection that is to blame (though it can be), but rather a lack of the body winding down the acute innate immune response, which instead persists far longer than it should.
Trials by DrHeyman’s group in 7,000 patients have shown that with the right treatment, patients undergo measurable epigenetic changes in their mitochondria and Transcriptome, their symptoms improve, and changes also occur in other objective pathology markers.
CIRS (biotoxin) is currently considered to be a chronic condition that lasts more than 6 months with abnormal pro inflammatory activity of Th1, Th2, Th17, coagulation pathways and complement activation. The reasons genetics make a difference is because it is thought CIRS is caused by a chronic Innate Immune response to antigen detection without proper presentation. (The immune system gets stuck in 1 phase of the process of dealing with a potentially infectious exposure). This also explains why many markers of inflammation may be normal even though there are many indirect measures revealing a pro inflammatory state.
For example, some markers that have been used are MSH (a regulatory neuropeptide), C4a (split product of C4a), MMP9 (only reliable way to measure Th1), ADH/osmolality (loss of feedback), ACTH/cortisol (loss of feedback and abnormal hormone control), NeuroQuant brain MRI analysis, cardio respiratory investigations (PFT, diffusion capacity, ECG and stress echo, VO2 max), Visual Contrast Study, and mitochondrial Transcriptomics[4,5].
The Department of Health in a committee review on the 8th of October 2018 observed commonalities between many symptoms of CIRS and those associated with CFS and Lyme disease. 56
The Royal Australasian College of Physicians (RACP) in their submission to the Australian Parliament’s Health, Aged Care and Sport Committee Inquiry into Biotoxinrelated Illnesses in 2018 said: "Other terms have been used in the literature including ‘multiple system multiple symptom multi-factorial conditions’ which are then sub-categorised by the dominant feature of their clinical presentation and/or a proposed relevant exposure. This is best exemplified by the body of work undertaken by the US Departments of Veteran Affairs and Defence in addressing what they termed ‘Chronic Multisymptom Illness’ (CMI). There are many overlapping features of CMI with those described by others as CIRS."
A recent Australian study found symptoms attributed to living in damp housing can persist for months to years, regardless of length of time exposed.
Reported symptoms associated with CIRS include combinations of things like:
- Fatigue
- Weakness
- Aches
- Muscle cramps
- Sharp pain
- Headache
- Light sensitivity
- Joint pain
- Morning stiffness
- Memory issues
- Difficulty with focus/concentration
- Word finding difficulties
- Decreased assimilation of new knowledge
- Confusion
- Disorientation
- Skin sensitivity
- Mood swings
- Sweats (especially night sweats)
- Temperature regulation or dysregulation problems
- Vertigo/Dizziness
- Red eyes
- Blurred vision
- Tearing
- Sinus problems
- Cough
- Shortness of breath
- Excessive thirst despite frequent water intake
- Static shocks
- Numbness
- Tingling
- Metallic taste
- Abdominal pain
- Diarrhoea
- Tremors 50
- Unusual pain 51
- Migraine/facial pain 52
- Appetite swings 53
- Increased urination 54/ nocturia 55
- Sensitivity to electromagnetic fields like mobile phones
Common misdiagnoses given to CIRS patients include:
- Chronic Fatigue Syndrome (CFS)
- Fibromyalgia
- Somatization (such as Hypochondria)
- Attention Deficit Hyperactivity Disorder (ADD/ADHD
- Depression and Anxiety
- Allergies
- Irritable Bowel Syndrome (IBS)
- Post-traumatic Stress Disorder (PTSD)
References
[1] Akin, C, Mast cell Activation Sydnromes - an overview
Akin C, Valent P, Mast cell activation syndrome: Proposed diagnostic criteria
Akin C., Mast cell activation syndromes., J Allergy Clin Immunol. 2017 Aug;140(2):349-355,
Sibilano R, Frossi B, Pucillo CE., Mast cell activation: a complex interplay of positive and negative signaling pathways., Eur J Immunol. 2014 Sep;44(9):2558-66.
Valent P, Akin C, Proposed Diagnostic Algorithm for Patients with Suspected Mast Cell Activation Syndrome, Journal of Allergy and Clinical Immunology, April 2019 Volume 7, Issue 4, Pages 1125–1133.e1
Yu Y, Blokhuis BR, Garssen J, Redegeld FA., Non-IgE mediated mast cell activation, Eur J Pharmacol. 2016 May 5;778:33-43.
[2] Brewer, JH, Thrasher JD, Straus DC, Madison RA, Hooper D. Detection of mycotoxins in patients with chronic fatigue syndrome, Toxins 2013; 5:605-617
Brewer JH, Thrasher JD, Hooper D. Chronic illness associated with mold and mycotoxins: Is naso-sinus fungal biofilm the culprit? Toxins 2014; 6:66-80
Brewer JH, Hopper D, Muralidhar S Intranasal antifungal therapy in patients with chronic illness associated with mold and mycotoxins: an observational analysis GJMR 2015 volume 15 issue 2: 29-33
Brewer, JH, Hooper, D & Muralidhar, S Intranasal Nystatin Therapy in Patients with Chronic Illness Associated with Mold and Mycotoxins Global Journal of Medical Research: K Interdisciplinary Vol. 15, Iss 5, 2015
Campbell AW, Thrasher JD, Gray MR, Vojdani A. Mold and mycotoxins: effects on the neurological and immune systems in humans. Adv Appl Microbiol. 2004;55:375-406. doi: 10.1016/S0065-2164(04)55015-3. PMID: 15350803.
Extract from Europe World Health Organisation (WHO) Guidelines for Indoor Air Quality: Dampness and Mould, 2009, full report here
Guilford, F, Hope, J, “Deficient Glutathione in the Patho-Physiology of Mycotoxin-Related Illness” Toxins 2014 6, pp. 608-623.
Hooper DG, Bolton VE, Guilford FT, Straus DC. Mycotoxin detection in human samples from patients exposed to environmental molds. Int J Mol Sci. 2009 Apr 1;10(4):1465-75. doi: 10.3390/ijms10041465. PMID: 19468319; PMCID: PMC2680627.
Lieberman SM, Jacobs JB, Lebowitz RA, Fitzgerald MB, Crawford J, Feigenbaum BA. Measurement of mycotoxins in patients with chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2011 Aug;145(2):327-9. doi: 10.1177/0194599811403891. PMID: 21493263.
Ponikau JU, Sherris DA, Kern EB, Homburger HA, Frigas E, Gaffey TA, Roberts GD. The diagnosis and incidence of allergic fungal sinusitis. Mayo Clin Proc. 1999 Sep;74(9):877-84. doi: 10.4065/74.9.877. PMID: 10488788.
Rea WJ, Didriksen N, Simon TR, Pan Y, Fenyves EJ, Griffiths B. Effects of toxic exposure to molds and mycotoxins in building-related illnesses. Arch Environ Health. 2003 Jul;58(7):399-405. doi: 10.1080/00039896.2003.11879140. PMID: 15143852.
[3] Dr. Patricia Kane, NeuroLipid Research Foundation
[4] Ritchie C. Shoemaker, Andrew Heyman, Annalaura Mancia, and James C Ryan. Inflammation Induced Chronic Fatiguing Illnesses: A steady march towards understanding mechanisms and identifying new biomarkers and therapies. Internal Medicine Review. October 2017.
[5] Ritchie C. Shoemaker and James Ryan. RNA-Seq on patients with chronic inflammatory response syndrome (CIRS) treated with vasoactive intestinal peptide (VIP) shows a shift in metabolic state and innate immune functions that coincide with healing. Medical Research Archives, Volume 4, Issue 7.